In medical literature and clinical practice, desmoid tumors may also be referred to as aggressive fibromatosis, desmoid-type fibromatosis, or deep fibromatosis
Atif Hussein, MD
Program Director, Hematology Oncology Fellowship Program
Memorial Cancer Institute
Hollywood, Florida
Desmoid tumors can pose a significant burden for patients. In my practice, I follow the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recommendations for initiating treatment when my patients have worsening symptoms, tumor growth documented on imaging, or impairment of functioning or daily activities.
Desmoid tumors can pose a significant burden for patients. In my practice, I follow the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recommendations for initiating treatment when my patients have worsening symptoms, tumor growth documented on imaging, or impairment of functioning or daily activities.
Atif Hussein, MD
Program Director, Hematology Oncology Fellowship Program
Memorial Cancer Institute
Hollywood, Florida
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Soft Tissue Sarcoma V.3.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved. Accessed March 13, 2026. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
Dr Atif Hussein is a paid consultant of SpringWorks Therapeutics, Inc.
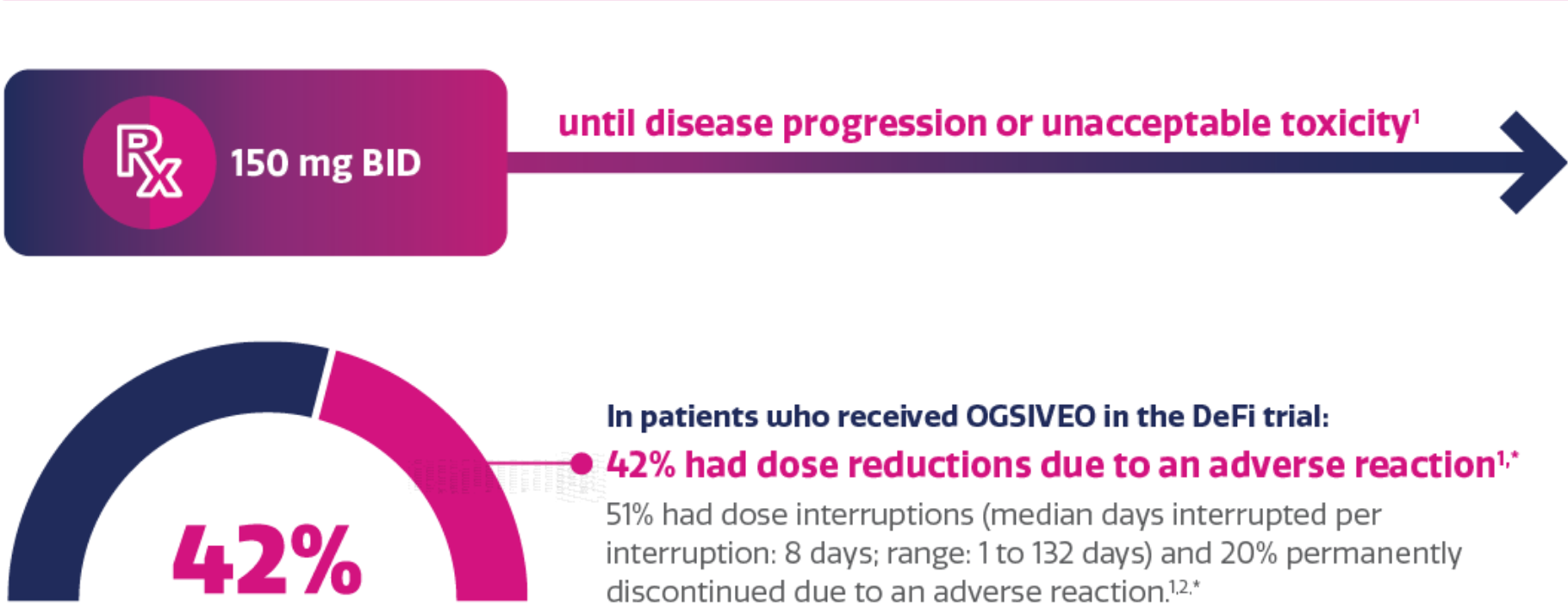
Patients with desmoid tumors may face uncontrollable growth and a high symptom burden1-4
Even though they do not metastasize, desmoid tumors often interfere with everyday activities and can be life-threatening1,2
Desmoid tumor characteristics:2,3,5,6
Rare
Locally aggressive
Unpredictable clinical course
Vital organs can be impacted
Desmoid tumors are associated with a potentially high and multifaceted burden of illness:4,*
Pain
Disfigurement
Decreased physical function
In focus groups and interviews, patients reported that pain was the most debilitating symptom of desmoid tumors1,†
Data from a Memorial Sloan Kettering/Desmoid Tumor Research Foundation patient-reported outcome (PRO) validation study that included patients with desmoid tumors (n=31, age range 20-68, 77% female). Patients participated in 60-minute qualitative phone interviews to provide their perspectives on disease symptoms and impact on their quality of life. The majority of the patients in this study were symptomatic (84%). Tumor site and type varied across patients. The concepts discussed during interviews were used to develop a draft patient-reported outcome scale, which was further refined in cognitive interviews of additional patients with desmoid tumors (n=15).4
Twenty-seven patients with desmoid tumors were interviewed from the Royal Marsden Hospital in the United Kingdom. Two focus groups and 13 interviews explored health-related quality of life issues and experiences of health care related to their desmoid tumors.1
Examples of desmoid tumors and potential symptoms
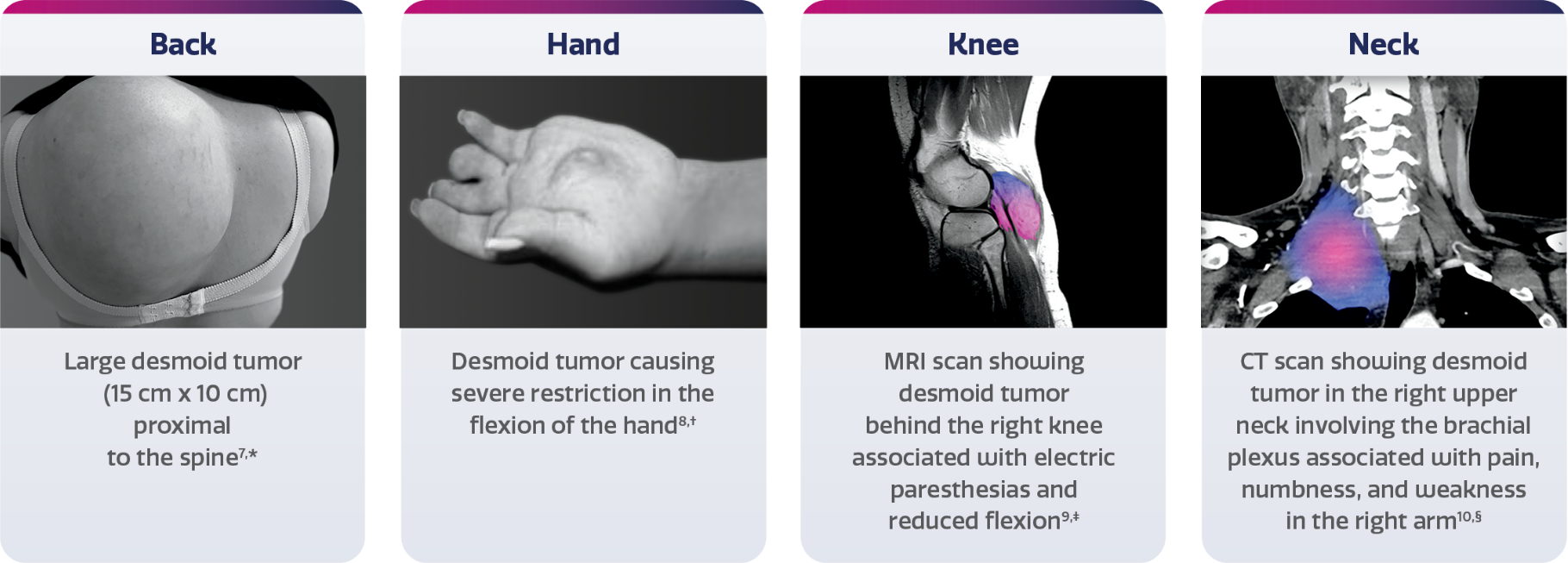

Image adapted from Cohen S, et al. World J Surg Oncol. 2008;6:28. Reused under Creative Commons License 2.0 (https://creativecommons.org/licenses/by/2.0). Image background changed to gray.
Image reproduced from Scaramussa FS, et al. SM J Orthop. 2016;2(3):1036. Reused under Creative Commons License 4.0 (https://creativecommons.org/licenses/by/4.0).
Image adapted from Weschenfelder W, et al. Case Rep Surg. 2015;2015:262654. Reused under Creative Commons License 3.0 (https://creativecommons.org/licenses/by/3.0). False color added.
Image adapted from Styring E, et al. Am J Med Case Rep. 2019;7(3):36-40. Reused under Creative Commons License 4.0 (https://creativecommons.org/licenses/by/4.0). False color added.
CT, computed tomography; MRI, magnetic resonance imaging.
References: 1. Husson O, Younger E, Dunlop A, et al. Desmoid fibromatosis through the patients’ eyes: time to change the focus and organisation of care? Support Care Cancer. 2019;27(3):965-980. 2. Constantinidou A, Scurr M, Judson I, Litchman C. Clinical presentation of desmoid tumors. In: Litchman C, ed. Desmoid Tumors. Springer; 2012:chap 2. Accessed October 4, 2024. https://www.researchgate.net/publication/226455135 3. Kasper B, Baumgarten C, Garcia J, et al. Desmoid Working Group. An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma Patients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann Oncol. 2017;28(10):2399-2408. 4. Gounder MM, Maddux L, Paty J, Atkinson TM. Prospective development of a patient-reported outcomes instrument for desmoid tumors or aggressive fibromatosis. Cancer. 2020;126(3):531-539. 5. Penel N, Chibon F, Salas S. Adult desmoid tumors: biology, management and ongoing trials. Curr Opin Oncol. 2017;29(4):268-274. 6. Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives. Pathologica. 2021;113(2):70-84. 7. Cohen S, Ad-El D, Benjaminov O, Gutman H. Post-traumatic soft tissue tumors: case report and review of the literature a propos a post-traumatic paraspinal desmoid tumor. World J Surg Oncol. 2008;6:28. 8. Scaramussa FS, Castro UB. Desmoid tumor in hand: a case report. SM J Orthop. 2016;2(3):1036. 9. Weschenfelder W, Lindner R, Spiegel C, et al. Desmoid tumor of the popliteal fossa during pregnancy. Case Rep Surg. 2015;2015:262654. 10. Styring E, Ahlstrom M, Rissler P, et al. Desmoid fibromatosis in the brachial plexus mimicking an ulnar nerve entrapment. Am J Med Case Rep. 2019;7(3):36-40.